941 was responded to the south for a central gun shot wound. O/A found a 20 year old male with a single small calibre gunshot wound to the left chest, 3rd intercostal space mid clavicular line with no exit wound.
The patient was GCS 15 but hypotensive and tachycardic. Pt also had some hemoptysis and were short of breath. SPO2 was normal. Breath sounds were clear with equal air entry. Pt was prepared for bilateral chest decompression prior to arrival of medical team.
Following the arrival of the medical team RSI and a digital thoracotomy were performed. While this was done I closely monitored the patients vital signs. It was at this stage that I noticed something unusual that neither the SCAT paramedic, the Doctor or I could explain. I noticed that the patient only had a radial pulse for every second QRS complex. The patient was monitoring in a sinus tachycardia and his central pulses matched the ECG. Furthermore the patients BP varied wildly. The patient’s BP swung from 80 systolic to 200 systolic and back again with no change to patient condition. The patients BP continued to do this throughout the case.
The Doctor performed an ultra sound of the chest but it did not show anything significant.
The patient was transported to St George where during surgery it was discovered that the patient had a large posterior pericardial tamponade.
Weeks later I was reading a case study at: http://lifeinthefastlane.com/cardiovascular-curveball-006/ when I realised what the strange presentation of this patient meant. Knowing this we could have diagnosed a pericardial tamponade even though it did not show up on ultra sound either on scene or in ED.
The first clue to a pericardial tamponade was the patient’s ECG. The patient’s ECG demonstrated Electrical Alternans. (Below is not the actual ECG)
Electrical Alternans are:
when consecutive, normally-conducted QRS complexes alternate in height.
produced by the heart swinging backwards and forwards within a large fluid-filled pericardium.
The second clue to a pericardial tamponade was the patients swinging BP.
I believe the patient was exhibiting a massive Pulsus Paradoxus.
Pulsus paradoxus is defined as an inspiratory drop in blood pressure of 10mmHg or more during normal breathing (http://lifeinthefastlane.com).
The number one cause of pulsus paradoxus is pericardial tamponade.
(Another case from Sydney HEMS showing a swinging BP from art line monitoring in accordance with the respiratory cycle, due to pericardial tamponade. SPO2 trace inaccurate due to helicopter vibration)
The third and most obvious clue to a pericardial tamponade was that the patient had a gunshot wound to the left chest (at least I picked up on that clue).
The patient made a full recovery and was discharged from hospital only days later. However if any of us on scene had recognised these signs, a pericardiocentesis could have been performed, resolving a life threatening situation.
My initial training as a Paramedic (and I’m sure this reflected by most others) was that in the setting of any suspected ischaemic cause to chest pain(and especially in a confirmed STEMI) high follow oxygen should be placed immediately onto the patient. Non rebreathers were standard care for MI. The biological plausibility model went along the lines of increasing the partial pressure of O2 in the alveoli would therefore super saturate the plasma, even though the SPO2 was already almost 100%. Reduced bloodflow through stenotic coronary arteries would have the maximum amount of O2 to deliver to ischaemic myocardial tissue.
Certainly sounded plausible to me at the time.
However in recent years there has been a lot of talk about potential harm of oxygen in these patients. So let’s review the evidence.
A few years ago the Cochrane Collaboration published a systematic review on Oxygen and AMI, available below:
The accumulated numbers from three included trials were not seen to gain full statistical significance, however potential harm was a derived assumption, and no benefit was seen from O2 administration.
These trials involved a total of 387 patients of whom 14 died. Of those who died, nearly three times as many people known to have been given oxygen died compared to those known to have been given air.
441 patients were considered for endpoint analysis. The Swedish study mentioned on the scancrit post is deto2x, a Swedish RCT aiming to recruit 6600 normoxic patients with AMI to 6lpm or air. The results of this will be very interesting!
QAS Drug Therapy Guideline for Oxygen: very comprehensive guide to treatment.
With the evidence accumulating against using O2 in AMI, how do we go about changing our ‘dogma’ and improving our practise for the good of patients?
The following cross sectional study of UK health providers found 98.3%(n=524) routinely or always use oxygen for AMI or ACS, and only 1.3% believed there was any association of it’s use and increased mortality.
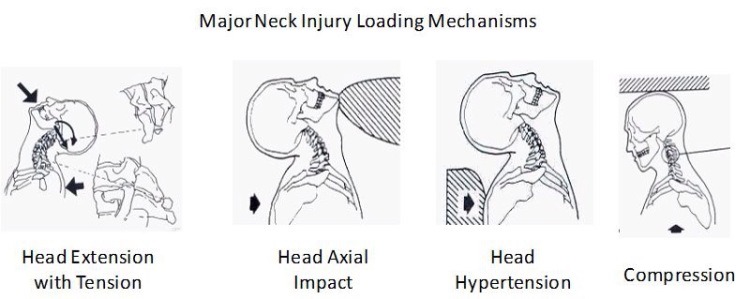
Prehospital Spinal Care – Are we doing the right thing by our patients?
First stop: Queensland Ambulance Service is getting rid of hard collars and using only soft collars very soon. Check out this post from Minhn Le Cong(QAS Royal Flying Doctors):
And one from the states that is an excellent overview, including a run down on the complications and issues that collars cause such as increased ICP, pressure sores, airway problems and increased movement of unstable cervical fractures:
There has been a recent update to the NSW Ambulance skills manual with a series of spinal precautions and immobilisation skill sheets. Take this consensus statement on minimal patient handling into consideration in conjunction with the new skill sheets:
Biomechanical analysis of various spinal immobilisation and extrication techniques, showing the worst in terms of shift of the spine from mid line was to use a NIEJ, strip the B pillar and extricate on a spineboard. The best technique was instruct the the patient to carefully step out of the vehicle, followed by application of a collar and then instruct to step out of the vehicle.
Investigates the spinal immobilisation of elderly patients with femoral/pelvic fractures caused by falls from sitting or standing height, finding only 0.4% incidence of spinal fractures out of 2441 patients. Many of these patients are collared due to their distracting injury.
Collars in penetrating trauma:
PHTLS Recommendations: – There are no data to support routine spine immobilization in patients with penetrating trauma to the neck or torso. – There are no data to support routine spine immobilization in patients with isolated penetrating trauma to the cranium. – Spine immobilization should never be done at the expense of accurate physical examination or identification and correction of life-threatening conditions in patients with penetrating trauma. – Spinal immobilization may be performed after penetrating injury when a focal neurologic deficit is noted on physical examination although there is little evidence of benefit even in these cases.
GSW to torso only caused injury via direct penetration of the spinal cord by a bullet, no benefit to be gained from collaring these patients, but a potential increase in scene time by 5.5 minutes on average and a worsening of airway issues which killed 16% of theses patients.
“Of particular concern are two studies that suggest an increase in mortality from spine immobilization in victims of penetrating injury.20,33 Vanderlan et al.20 reviewed data from a single trauma center and noted cervical collar placement to be an independent risk factor for death. An analysis from the National Trauma Data Bank of 45,284 patients with penetrating trauma noted a twofold increase in mortality in patients who were immobilized compared with similar patients who were not.33 Only 0.01% of patients with an incomplete spinal cord injury eventually required operative spine fixation, leading the authors to conclude that spinal cord damage from penetrating trauma is done at the time of injury, does not worsen, and does not benefit from immobilization. The increased mortality found in immobilized patients was attributed to increased scene times and the potential to miss signs of immediate life threat, such as tracheal deviation and subcutaneous emphysema.”
9 cadavers, collar application effectively “pushed” the head away from the shoulders, causing gross separation of high cervical injury by displacing the verterbral gap at the site of injruy.
Small sample size of 7 “fresh” cadavers, however found significant movement of the C-spine with collars on during log rolling and other patient movement. Postulated that a pivot point is caused by the collars plastic.
5 cadavers(not so fresh this time) with 2 different types of collars or no collar, found very little reduction in movement across the groups. Suggest that collars provide a visual cue but very little other benefit.(This is in line with the goals of QAS soft collars, almost no reduction in movement of the spine but provide a visual cue and also reduce the negative effects of hard collars).
Patients injured in IED blasts had a 10.4% incidence of acute spinal injury(n=212), higher than that from other blunt force mechanisms in the study. Blast injury patients were also significantly less likely to have spinal precautions in place.
Link to an earlier format: *some links no longer working* of the clinical focus on cardiac arrest centres, post ROSC cooling, “down time”, advanced airways in OHCA and the START trial.
Check out the paper up at station(and linked below) on the CHEERS trial being run down in Melbourne with The Alfred, 54% of patients so far walking out of hospital with no neurological deficits! Could well be the future of OHCA care.
This post will cover a case study from a recent job followed by a rundown of our protocol for diving emergency, some background for why we treat the way we do and then some further pathophys and definitive treatment.
A recent job on the Northern Beaches:
Called to a 34 YOF diver pulled out of the water after a ‘deep dive’, agitated and on the way in to a boat ramp for RV with ambulance.
O/A the charter dive boat was just about to pull in, 1 diver made his way to the shore and said the patient was on O2 but was so combative that she was very hard to manage and that he thought this may be due to the fact she suffers from vertigo.
Once we extricated with the boat crews help to the beach we lay her R lateral and directed her to stay flat with her head down, and not to sit up or raise her head for any reason. One paramedic stayed at her head and held the NRB on high flow to her face whilst I cut the sleeves off her wetsuit, gained IV access and collected as much dive profile history as possible.
Dive profile:
Experienced diver, nil recent trauma or illness. First and only dive for the day.
68 min under, 26 min at max depth of 45m.
Full decompression with 3 stops at 9, 6 then 3m; with air, 50% O2 then 100% O2.
Noted to have ?convulsions as ascending from the 3m stop, pulled limp from the water and immediately put on O2, becoming more responsive but agitated.
The primary survey was as follows:
R – GCS 14, agitated
A- clear, boat crew stated she had been frothing on the way in
B- Grossly tachypnoeic, upwards of 50/min, SPO2 89%
C- Tachycardic, 140/min
D- pain to knees, chest pain, nil neck pain or headache, nil signs or history of trauma, PEARL
E- double wetsuit on, temp 36.8
Once loaded we Tx R1 to POW in Randwick to access the hyperbaric chamber, and on the way asked the control centre to contact the Dive Medicine Unit at Balmoral to query access to their chamber. This was knocked back and we continued to POW with a code 3.
With oxygenation the patient quickly calmed and became GCS 15. Her obs stabilised and 750ml of hartmann’s was administered over the journey, with pain relief declined. A persistent dry cough worsened and by arrival at the ED had become productive with blood stained sputum. Her resp rate stayed at 50/min and her heart rate came down to 115/min ST. She had nil signs of a pneumothorax and was mildly hypertensive throughout.
After handover the patient was confirmed to have pulmonary oedema and was placed on CPAP. The hyperbaric consultant arrived and made the point that the dive history is his single most important tool to differentiate symptoms and decide on further treatment. He also asked to speak to the dive buddy, and we accessed the callback to put him onto the boat skipper to confirm the details. This was a good learning point that apart from gaining an extensive dive profile it is handy to bring a dive buddy or keep phone details for further questioning.
The patient was heading down to the chamber shortly after.
Diving Emergencies Protocol:
Basic patient care – Including extensive and accurate dive profile
Posture supine – Post barotrauma an Arterial Gas Embolism(AGE) can travel into the cerebral vasculature causing stroke like symptoms, keeping the patients head down can aid in preventing this.
Administer 100% O2
Treat pneumothorax if present – Barotrauma(remember Boyles Law?!) from the gas expanding in the lungs as the patient ascends and the atmospheric pressure drops, especially if breath is held, can rupture the pleura
Hartmann’s – Dry gas, salt water, exertion and a responsive diuresis to increased blood volume combine to cause dehydration in these patients, get fluids in early.
Pain management – Pain can be caused by nitrogen bubbles in the joints or through the pulmonary vasculature. Tooth, sinus, facemask or ear pain are also common from expansion of gas filled cavities.
Prevent hypothermia – leave wetsuit on – Obvious one, water=cold! In my recent case I elected to only expose the arms however there is merit in further exposure, especially if the patient is displaying signs of deterioration; as assessment and treatment for subcutaneous emphysema and decrease in air entry will be hindered by having the wetsuit over the thorax.
Contact a centre experienced in diving emergencies through the control centre – POW is the only Dive Medicine Unit we can access in Sydney, however there is a hotline if you need quick info for the Dive Emergency Service at the Royal Adelaide, with 24 hour access to a dive medicine specialist. The number is 1800 088 200 and it will be taken by the SA Ambulance Service call takers, then transferred to a doctor.
Urgent transport
Suspect decompression illness in any patient who presents within 24 hours of a dive – Especially maintain a high index of suspicion in a patient that has flown in the day or two after a dive, the effects of going up to an even higher altitude than sea level obviously exacerbate the problem!
Remember that signs and symptoms can be highly variable; therefore you must maintain a high index of suspicion with any clinical presentation
This is a great paper published last year with a thorough rundown on the pathophysiology of diving emergencies and further treatment:
4. Briefly suction mouth and pharynx under direct vision if secretions are present
5. CPR including airway management if heart rate <60/min, despite ≥30 seconds of
ventilation. Compressions should continue until heart rate >60/min and increasing
Ratio 3 compressions to 1 ventilation
(90 compressions: 30 inflations/min)
* A video from SMACC on resus of the newborn:
6. Repeat APGAR at 5 minutes, and every 5 minutes till APGAR >7
7. Adrenaline if HR <60/min despite effective CPR
8. Treat associated conditions if present:
– Hypoperfusion/hypotension
– Hypoglycaemia
9. Prevent Hypothermia
10. Urgent Transport if unresponsive to treatment
Adrenaline 10mcg/kg IV/IO every 4 minutes
– Indication: HR<60/min despite effective CPR
Hartmann‘s 10ml/kg IV/IO bolus
– Indication: Failure to respond to CPR and adrenaline
Glucose 10% 0.25ml/kg IV/IO bolus
– Indication: BGL <3mmol/L
A couple of videos on neonatal intubation and meconium suction:
The second one covers some basic stuff but has some great views of neonatal airways:
Placental Abruption:
This guys a bit annoying but this video is a good simple rundown of this time critical obstetric emergency:
And a simplistic rundown to help visualise the complications of Abruption, highlighting the need to be ready to treat for hypovolaemia and maintain endorgan perfusion
– rectal pressure: urge to move bowels or pass gas
– confusion, restlessness
– increased bloody show
– trickle or gush of amniotic fluid
Signs of Imminent delivery:
– Urge to bear down, move bowels, or push that is irresistible
– Increased bloody show
– Bulging of perineum
– Dilation of rectal sphincter
Delivery: One person takes charge, others play gofer as needed. Clear out non-helpful bystanders. Keep calm, keep voice low. Set up clean area that won’t accidentally get messed up by mother. Lay out all necessary equipment, set up oxygen. Wash hands and arms if there is time. Place clean drape under mother’s buttocks (be prepared for gofer to clean away feces if necessary)
Explain to mother what is happening, as it happens. As the perineum bulges, place hand gently but firmly over the introitus and the perineum, to prevent sudden uncontrolled expulsion of the fetal head. Encourage the mother to pant or push very gently, explaining you want to avoid a tear.
As the head emerges, keep firm gentle pressure on head and perineum until chin delivers. Feel for the cord behind the top ear. If found, gently tug to see if it will slip over the head. If tightly wrapped, clamp in 2 places and cut between.
Suction the baby’s mouth and nose. This is mainly important if the amniotic fluid is green or brown colored. Otherwise it’s probably not a vital step and can actually cause breathing problems. [Note – It is important to suction the mouth before the nose. “The mouth is suctioned first to ensure that there is nothing for the infant to aspirate if he or she should gasp when the nose is suctioned.” [From the AAP/AHA Textbook of Neonatal Resuscitation, rev. 3/95, p. 2-12.]
After head rotates to face mother’s thigh, gently press down on head to encourage the top shoulder to deliver. When you can see the baby’s top armpit crease, lift up on the head to deliver the bottom shoulder. The rest of the baby should follow.
Suction the baby’s mouth and nose. Dry the baby vigorously, then DISCARD WET TOWELS and wrap the baby in dry warm clothes or blankets.
Administer oxygen at 5 liters 1 1/2 inch from baby’s face until trunk is pink and hands and feet less blue. Some cyanosis of extremities is expected. Keep rest of baby’s trunk and head well covered while administering oxygen as the draft will chill the child. If not expected to get to the hospital soon, clamp and cut the cord 10-15 minutes after the birth. (clamp the cord about 3 inches from the abdomen, then 2 inches beyond that, and cut between the 2 clamps.)
Place the baby on mother’s chest, with head lower than feet to allow gravity to assist the baby in clearing the airway.
Watch for sudden gush of blood and lengthening of cord. This means placenta has detached and is ready to be born. Provide gentle traction on the cord. Placenta will usually be pushed out easily by mother. If it doesn’t, get to hospital as soon as possible. Normally, approximately one cup of blood is generally lost with the delivery of the placenta. After placenta born, immediately press fingers slowly and gently into abdomen at umbilicus – you’ll feel the top of the uterus. It may be somewhat spongy or slightly firm or rock hard if she’s having a contraction. Do slow and gentle circular massage to encourage contraction of the uterus. This is extremely important, especially if there’s a constant flow of blood.
Cutting the cord:Late clamping of the umbilical cord is a physiological and inexpensive means of enhancing hematologic status, preventing anemia over the first 3 months of life and enriching iron stores and ferritin levels for as long as 6 months. Although this is of particular importance for developing countries in which anemia during infancy and childhood is highly prevalent, it is likely to have an important impact on all new-borns, regardless of birth setting.
Hutton, E. K., & Hassan, E. S. (2007). Late vs early clamping of the umbilical cord in full-term neonates: systematic review and meta-analysis of controlled trials. Jama, 297(11), 1241-1252.
The results suggest a beneficial effect of late cord clamping, produced by an increase in antioxidant capacity and moderation of the inflammatory-mediated effects induced during delivery of term neonates.
Díaz-Castro, J., Florido, J., Kajarabille, N., Garrido-Sánchez, M., Padilla, C., de Paco, C., … & Ochoa, J. J. (2014). The Timing of Cord Clamping and Oxidative Stress in Term Newborns. Pediatrics, 134(2), 257-264.
A more liberal approach to delaying clamping of the umbilical cord in healthy term infants appears to be warranted, particularly in light of growing evidence that delayed cord clamping increases early haemoglobin concentrations and iron stores in infants. Delayed cord clamping is likely to be beneficial as long as access to treatment for jaundice requiring phototherapy is available.Effect of timing of umbilical cord clamping of term infants on mother and baby outcomes At the time of birth, the infant is still attached to the mother via the umbilical cord, which is part of the placenta. The infant is usually separated from the placenta by clamping the cord. This clamping is one part of the third stage of labour (the time from birth of the baby until delivery of the placenta) and the timing can vary according to clinical policy and practice. Although early cord clamping has been thought to reduce the risk of bleeding after birth (postpartum haemorrhage), this review of 15 randomised trials involving a total of 3911 women and infant pairs showed no significant difference in postpartum haemorrhage rates when early and late cord clamping (generally between one and three minutes) were compared. There were, however, some potentially important advantages of delayed cord clamping in healthy term infants, such as higher birthweight, early haemoglobin concentration, and increased iron reserves up to six months after birth. These need to be balanced against a small additional risk of jaundice in newborns that requires phototherapy.
McDonald, S. J., Middleton, P., Dowswell, T., & Morris, P. S. (2014). Effect of timing of umbilical cord clamping of term infants on maternal and neonatal outcomes. Evidence‐Based Child Health: A Cochrane Review Journal, 9(2), 303-397.
Shoulder Dystocia: Occuring in about 2-7% of deliveries shoulder dystocia is the capture of the anterior shoulder under the symphisus pubis preventing progress of delivery. Simply incorporating the knees to chest position(McRoberts Manouevre) can provide up to 42% success in this presentation, especially with some suprapubic pressure to assist. The video below goes through what to do if this is not successful, take note of the high mortality rate if undelivered within 5 minutes:
an actual breech delivery, note the use of lovesets manoeuvre to release the arms and the modified maurcieau smellie viet technique(baby on the forearm to release the occiput)as shown in the video above. Start watching from 3 min.
More advanced treatment in a more time critical situation is to push the presenting part gently off the cord:
Our treatment – Position left lateral with buttocks elevated
– Pillow between legs to relieve pressure
– Do not handle cord
– 100% O2 – Urgent Tx Primary Postpartum Haemorrhage PPH is greater than 500ml PV bleeding in the first 24hours post delivery. Signs of haemorrhagic shock can be hidden by the physiolgic changes of the mother during pregnancy, and a high index of suspicion should be maintained for a more serious bleed than might be obvious to the Paramedic. Plain language summary of the latest recommendations for PPH from: Mousa HA, Blum J, Abou El Senoun G, Shakur H, Alfirevic Z. Treatment for primary postpartum haemorrhage. Cochrane Database of Systematic Reviews 2014, Issue 2.
Treatment for excessive bleeding after childbirth After a woman gives birth, wombmuscles contract, clamping down on the blood vessels and helping to limit bleeding when the placenta has detached. If the muscles do not contract strongly enough, very heavy bleeding (postpartum haemorrhage) can occur, which can be life threatening. These situations are common in resource-poor countries, and maternal mortality is about 100 times higher than in resource-rich countries. It is a very serious problem that requires effective treatments that might avoid the use of surgery to remove the womb (hysterectomy). This is often the last treatment option and leaves the woman unable to have more children. In most settings, women are given a drug at the time of birth (before excessive bleeding occurs) to reduce the likelihood of excessive blood loss. However, despite this intervention, some women bleed excessively, and this review looked to see what interventions might be used to reduce the amount of blood lost by these women. Treatment options include drugs to increase muscles contractions (such as oxytocin, ergometrine and prostaglandins like misoprostol), drugs to help with blood clotting (haemostatic drugs such as tranexamic acid and recombinant activated factor VII), surgical techniques (such as tying off or blocking of the uterine artery) and radiological interventions (to assist in blocking the main artery to the womb by using gel foams). The review identified 10 randomised controlled trials involving 4052 women. Seven of these trials looked at a drug called misoprostol, which is a prostaglandin and so works by increasing muscle contractions. Overall, the trials suggest that misoprostol does not work as well as oxytocin infusion, and it has more side effects. However, oxytocin needs to be kept in a refrigerator, and so in settings where refrigeration and infusions are not readily available, misoprostol can be used. Other clinical trials looked into using other types of drugs or squeezing the main artery that supplies blood to the woman. The number of women included in these studies was too small for any useful conclusions regarding their effectiveness and safety. Whilst this cochrane review shows oxytocin and misoprostol as effective mediations in PPH, we don’t carry them, so urgent transport to hospital where they can be given is our main modallity of treatment. Thorough rapid assessment of signs of hypoperfusion and supportive therapies enroute are essential.
Secondary Postpartum Haemorrhage: Postpartum hemorrhage (PPH) represents serious problem for women and obstetricians. Because of its association with hemorrhagic shock and predisposition to dissemi- nated coagulopathy, it is a leading cause of maternal deaths worldwide [1]. The severity of PPH is potentiated by the fact that it is not specifically associated with the mode of delivery (vaginal vs. cesarean section). Furthermore, the jeopardy of PPH is rising with the secondary form of PPH (abnormal excessive bleeding from the birth canal, mostly uterus, occurring between 24 hours and 6 weeks postpar- tum), when women are already discharged home. PPH is a widely underestimated obstetric problem with variable occurrence and severity when diagnosed. This is caused by the lack of definitions and describing criteria used for this condition (e.g., quantification of blood loss, variable cutoff limits for estimated blood loss, and linkage to the mode of delivery). In general, the incidence of PPH is approximately 5%-20% of labors [1,2], with the highest rates in developing countries.The primary danger for patient is that bleeding in the majority occurs between 1 and 2 weeks after delivery when patient is often home and unaware that the hemorrhage is significant and potentially life threatening.
As an extension to the post earlier in the year on STEMI Equivalents, this month we’re going to look at the opposite: expanding on your knowledge of ECG patterns that may look considerably like a STEMI and quite possibly will be read by the algorithim in the Lifepak 15 as a STEMI, however may not indicate an acute coronary artery occlusion. Pericarditis is one that we all know to keep an eye out for, but less commonly taught mimics like Brugada and Benign Early Repolarisation are just as important.
Why should we even bother to recognise STEMI mimics? Whilst overtriage is better than undertriage, and we have a system in metro where the ECG is reviewed when we transmit it through, there are a number of reasons why we should be well practised at recognising mimics:
– Ongoing issues of false positive activation of cath labs will stretch resources and decrease faith in the interventional cardiology team of ambulance skill in STEMI recognition.
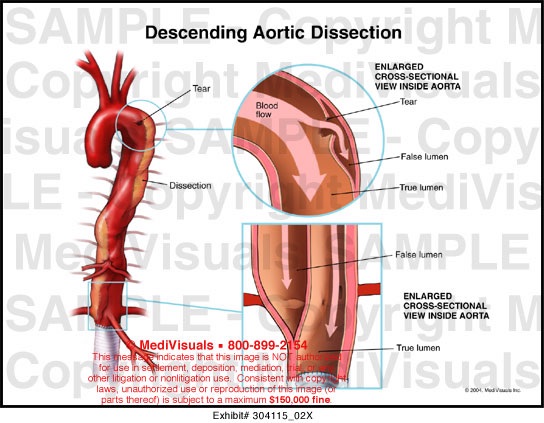
– Delayed treatment for the actual cause of the mimic: eg hyperkalaemia, aortic dissection.
– Iatrogenic harm: giving aspirin/GTN/morphine/fibrinolytics in regional areas for patients without acute occlusions. Also unwarranted angiography, although there are checks with transmission, it is more difficult for ED registrars and cardiologists to make a decision to cancel the activated cath lab once ambulance has sent an ECG through.
– Degrades perceptions of Paramedic skill, knowledge and professionalism.
Below are some explanations, diagrams and links on some of common and less common STEMI equivalents. Check it out, learn some of the patterns and don’t forget that we always work under the guidance of NSW Ambulance protocols, pharmacologies and SOP’s.
Lifepak 15 skill sheet states:
• All patients with suspected ACS must have a diagnostic quality 12 lead ECG acquired • Transmit ECG’S that state:
“MEETS ST ELEVATION MI CRITERIA” and / or “CONSIDER ACUTE INFARCT”
LBBB and Paced Rhythms
LBBB and paced rhythms present a challenge when differentiating them from a STEMI. Abnormal depolarisation in the setting of a pacemaker or aberrant conduction through the bundle branchs will result in abnormal repolarisation(T Wave) and therefore an abnormal ST segment. As opposed to STE in an AMI, STE from a LBBB is due to the conduction of repolarisation through an abnormal pathway. This is obviously the same in a paced rhythm.
So can we therefore say that if a patient shows a LBBB or pacemaker spike there is no acute coronary artery occlusion?
Unfortunately not. The LBBB may be new for the patient, and therefore the result of an AMI. And a patient with a pacemaker may have a ruptured thrombus causing an AMI however the pacemaker is firing so we cannot see whether there is a STEMI.
Trying to find out whether a LBBB is a new onset in the prehospital environment is almost impossible(usually done through review of old ECG’s), and turning off the pacemaker is not an option. This is where Sgarbossa’s criteria can be implemented to decide(refer previous post on STEMI equivalents). If an ECG is positive to sgarbossa’s criteria it is indicative of the need for urgent cath lab activation. Recall though that this criteria has been validated as highly specific but not particularly sensitive to the identification of STEMI, so a LBBB that presents with ischaemic symptoms should be treated with a high index of suspicion.
Traditionally new LBBB is considered a sign of AMI, however the paper below shows some recent research debunking this. LBBB are most commonly the result of underlying ischaemic or structural heart disease. If LBBB is the result of an AMI it is very likely that it will be a large area of the myocardium effected, and haemodynamic instability is a common finding.
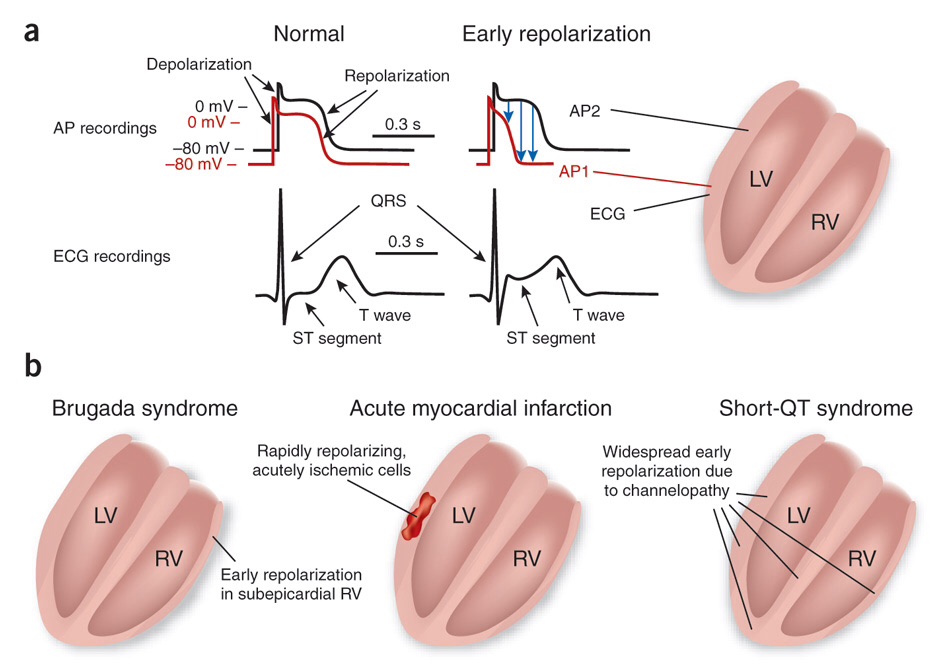
Early repolarization pattern (ERP) is a common ECG variant, characterized by J point elevation manifested either as terminal QRS slurring (the transition from the QRS segment to the ST segment) or notching (a positive deflection inscribed on terminal QRS complex) associated with concave upward ST-segment elevation and prominent T waves in at least two contiguous leads.1,2 The J point deflection occurring at the QRS-ST junction (also known as Osborn wave or J wave) was first described in 1938, and is seen in both extracardiac and cardiac disorders like hypothermia, hypercalcemia, brain injury, hypervagotonia, or spinal cord injury leading to loss of sympathetic tone, vasospastic angina. Besides recently described early repolarization syndrome, ERP has generally been considered a normal ECG variant with good long-term prognosis. However, this long-held concept has been challenged, and recently published population-based studies and reports of associations with ventricular fibrillation and sudden death continue to fuel more momentum.6–9 In the seminal article by Haïssaguerre et al, cases of ERP associated with cardiac arrest, had at least 0.1-mV J point elevation manifested as QRS slurring or notching in the 2 contiguous inferior or lateral leads.6 ERP has also emerged as a marker of increased long-term mortality (cardiac and arrhythmic) in the general population.10,11 Thus, ERP is probably not as benign as traditionally believed.
Nicolas Derval, MD; Ashok Shah, MD; Pierre Jaïs, MD, Definition of Early Repolarization:A Tug of War, Circulation, 2011; 124: 2185-2186.
Left Ventricular Hypertrophy
From Jems:
Left Ventricular Hypertrophy (LVH)
LVH is responsible for up to 30% of ST elevation.It’s defined as an increase in mass to the left ventricle, often in response to chronic hypertension. As the heart beats continuously against a higher diastolic afterload, cardiac tissue surrounding the left ventricle grows, stealing space, and thus volume, from its ventricle. The long-term prognosis for these patients is poor because the condition eventually leads to decreased diastolic and systolic function. These patients often develop close relationships with their cardiologists and emergency departments as cardiac function drops, and their risk of AMI and other cardiac disease climbs. As the left ventricle loses its ability to move blood, the pump backs up into the left atria and then into the lungs; many of our CHF patients will demonstrate the signature QRS pattern of LVH (see Figure 2). Exaggerated QRS complexes dominate the precordial leads, resembling the tracing of a large earthquake.
Note the prevalence of this mimic in STE… more than a quater of all ECG’s with elevation will be LVH! And follow this link for a brilliant explanation with examples:
Hyperkalaemia can cause many ECG changes and the common ones are taught to us in school, flattened/lost P waves, peaked T waves, widened QRS and sine wave. There are many more iterations of the effect of high potassium on the myocytes and there is a saying that if the ECG is ‘bizarre’ then it is hyperkalaemia. Check out the following blog post and some of the links within for more info on hyperkalaemia presenting as a STEMI mimic:
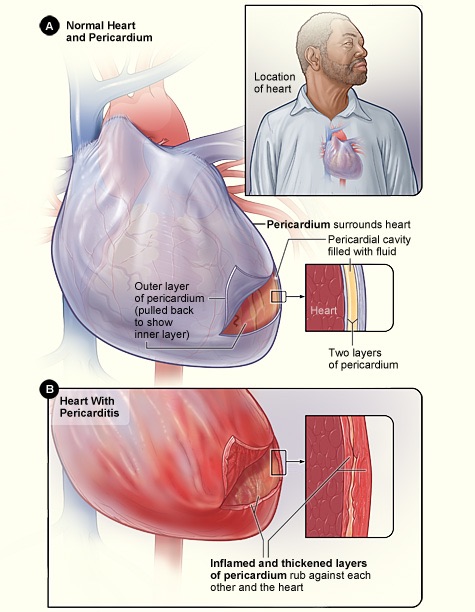
Pericaditis is an infection/inflamation of the pericardial sac and can cause ECG changes that mimic STEMI. The most important distinguishing factor is that the STE is not confined to an area of the heart and may be global or nearly global. Reciprocal changes as seen in a STEMI will also be absent. Your clinical assessment will play a large role as well, have a look at the table below to refresh your memory on distinguishing points on ischaemic versus pericarditis related chest pain.
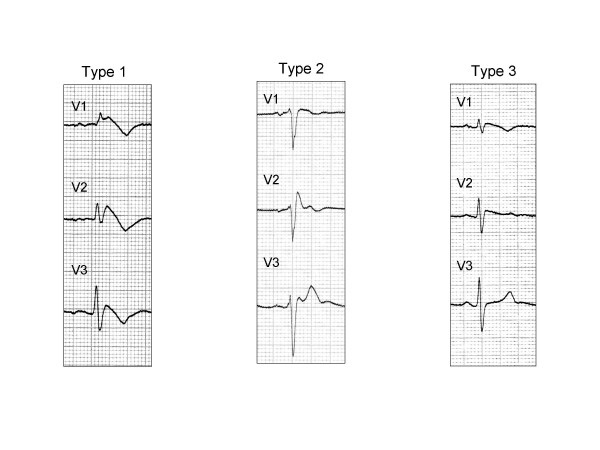
Brugada syndrome is reported to be present in 1 in 2000 people in the general population, and considerably more in the SE asian population. It is responsible for approximately 4% of sudden cardiac deaths through progression into VT.
Takotsubo
Takotsubo Cardiomyopathy
Angry octopus trying to escape a takotsubo!
The last mimic we’ll cover here is just for interests sake, as it is undistinguishable except by angiogram from AMI. I took a patient to RNSH last year with a clear STEMI on their ECG and it ended up being a ruptured ventricular wall, having a chat with the lady she had recently lost her husband and was under a considerable amount of stress. Hence why it is called ‘broken heart’ syndrome!
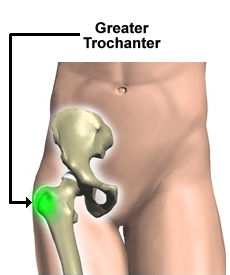
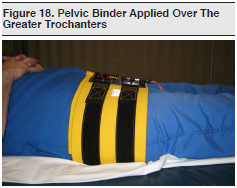
Whilst this video is of a specific pelvic device, the principles apply equally in our setting. And hopefully we can arrange a station visit by Sam Medic…
NSW Ambulance Pelvic Binding Skill Sheet:
Aim:
To reduce a pelvic fracture, provide mechanical stability to the pelvis, and reduce blood loss.
Indication
All trauma patients with any of the following
• signs of a pelvic fracture including pain in the pelvis, hip, groin or lower back; or
• signs of hypovolaemic shock; or
• suspicious mechanism of injury, even if currently haemodynamically stable
The application of pelvic sheeting has negligible adverse effects on those patients who are subsequently found did not sustain a pelvic fracture.
Applying it to fifty patients who didn’t need it is worth it for the one who does
High risk groups include:
• Motor vehicle crashes, especially with patient side impact
• Vehicle v pedestrian / cyclist
• Motor bike crash
• Crush or compressive force
• Patients > 65 years of age
• Fall from height
• Fallen from, trampled or crushed by livestock
Have an increased index of suspicion with:
• Patients with decreased level of consciousness
• Drug or alcohol affected
• Significant distracting injury
Pelvis MUST NOT be sprung or compressed, however pelvis should be gently palpated as part of
patient assessment.
ALWAYS apply pelvic sheeting when indicated, even in urgent transport situations.
Blood loss from pelvic fracture can exceed 2 litres – this needs to be mitigated as the highest priority to
prevent worsening shock.
Every 3 minutes of untreated hypotension causes mortality to rise by 1%.
Some guidamce on placement of the pelvic sheeting:
Main points from the literature review and consensus statement:
– A binder is a treatment not a packaging tool, apply it early.
– A pelvic binder should be applied prior to extrication.
– Log rolling should be avoided and a scoop used where possible, rolling only to 15 degrees to facilitate placement on the board.
– Binder should be placed as close to skin as practical.
– There is a high incidence of occult pelvic fracture and bleeding in the obtunded major trauma patient(76%), so a high index of suspicion should be maintained, and a binder considered whenever a collar is placed due to mechanism.
– Up to 35% of total blood volume can be lost into the pelvis before any change is noted in systolic blood pressure. Permissive hypotension should be practised, with the presence of a radial pulse being the endpoint for fluid resus in the blunt trauma patient with no closed head injury.
– Examination is unreliable, springing has been shown to have a sensitivity of only 59%. Combined with the risk inherent of exacerbating haemorrhage this procedure has no role in pelvic injury assessment.
This is a great video on the bleeding associated with pelvic fractures, watch just the first minute.:
Following are some resources on the T-Pod, a pelvic binding device used by SOT. The T-Pod is employed as it is light, can be applied by one operator and is useful in the setting of deployments and remote work. It is carried by SOT responders in all situations however it is primarily for use in remote or deployment environments. The following is some information on the device to gain some familiarity as you may see it around, Careflight 4 also use the T-Pod in Sydney.
This is a “mini” systematic review of the literature to assimilate evidence when there is not a huge amount of literature available. Findings are that pelvic binding devices commercially available all reduce pubic symphisis diastasis significantly:
A case series report showing application of the T-Pod reduces heart rate, increases blood pressure and reduces pelvic volume in trauma patients with unstable pelvic fractures. 15 patients included:































 </
</